

Introduction:
Previous literature suggests that allogeneic hematopoietic stem cell transplant (HCT) utilization rates are lower amongst Hispanic and Black compared to non-Hispanic White (NHW) cancer patients. However, no previous studies have focused explicitly on the pediatric and adolescent young adult (AYA) population. We sought to examine utilization of HCT by race/ethnicity using the California Cancer Registry (CCR) and the Office of Statewide Health Planning and Development (OSHPD) hospitalization database. We hypothesized that Black and Hispanic patients with acute leukemia less frequently receive HCT than NHW patients.
Methods:
Using population-based data from California, a retrospective cohort of patients aged 0-39 years with acute myeloid leukemia (AML) or acute lymphoblastic leukemia (ALL) diagnosed between 2000 and 2015 was assembled. The primary exposure was a composite of race/ethnicity with NHW patients as the reference group. The primary outcome was receipt of first HCT, defined by diagnosis codes in OSHPD or treatment in the CCR. Logistic regression analyses were used to estimate odds ratios (OR) and corresponding 95% confidence intervals (CI). Multivariable models were adjusted for race/ethnicity, age, sex, year of diagnosis, leukemia type, insurance type at diagnosis, rurality, and neighborhood socioeconomic status at diagnosis (SES).
Results:
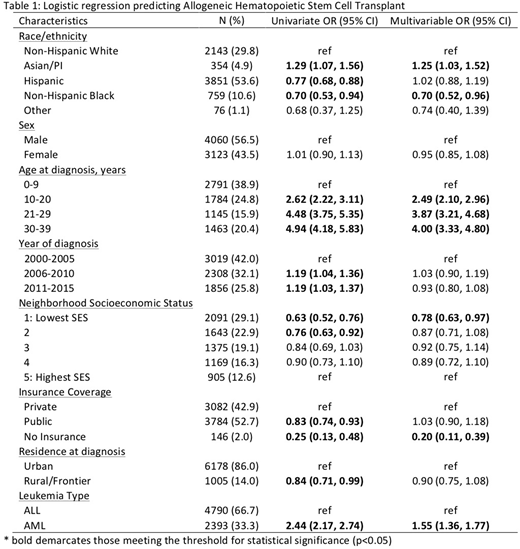
Among 7,183 patients (4,790 with ALL and 2,393 with AML), 21% (16% of ALL patients and 31% of AML patients) underwent HCT. Distributions of insurance type and neighborhood SES differed by race/ethnicity with a higher proportion of Black and Hispanic patients having Medicaid insurance and living in lower SES neighborhoods. In univariate analyses, Black and Hispanic race/ethnicity were associated with decreased likelihood of receiving HCT (OR 0.70 95% CI 0.53, 0.94 and OR 0.77 95% CI 0.68, 0.88, respectively) and Asian race was associated with increased likelihood of HCT (OR 1.29 95% CI 1.07, 1.56) compared to NHW patients. In the multivariable model, there was no statistically significant difference in receipt of HCT among Hispanic patients, but disparities persisted among Black patients (Table 1). Uninsured patients and those in the lowest SES quintile were also less likely to receive HCT, while older age and AML were associated with HCT receipt. In analyses stratified by age and leukemia type, we found that the disparities in receipt of HCT among Black patients was largely driven by patients >20 years old (adjusted OR 0.50 95% CI 0.33, 0.78). These analyses also revealed that the increased likelihood of HCT among Asian/PI patients was driven by patients <21 years old with ALL (adjusted OR 1.59 95% CI 1.07, 2.38). Among those who did undergo HCT, Hispanic patients had a longer initial HCT admission (39 v. 35 days, p< 0.0001) and more frequent readmissions (32% with >2 readmissions in the first year post-HCT v. 25%, p=0.005) compared to NHW patients.
Conclusions:
HCT is a potentially curative treatment for high-risk acute leukemia; thus the observed racial and SES disparities in receipt of HCT may contribute to disparities in leukemia survival. More detailed disease, treatment, and relapse data would provide a better understanding of the etiology of our findings and allow for reduction of existing disparities through improved access to HCT.
Muffly:Servier: Research Funding; Amgen: Consultancy; Adaptive: Research Funding. Wun:Glycomimetics, Inc.: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal